Treatment Volume

Home > Treatment Planning > Prescription & Dose Calculation > Treatment Prescription > Treatment Volume
Gross Tumor Volume:
The gross tumor volume (GTV) is the gross demonstrable extent and location of the tumor. It may consist of primary tumor, metastatic lymphadenopathy, or other metastases. Delineation of GTV is possible if the tumor is visible, palpable, or demonstrable through imaging. GTV cannot be defined if the tumor has been surgically removed, although an outline of the tumor bed may be substituted by examining preoperative and postoperative images.
Clinical Target Volume:
The clinical target volume (CTV) consists of the demonstrated tumor(s) if present and any other tissue with presumed tumor. It represents, therefore, the true extent and location of the tumor. Delineation of CTV assumes that there are no tumor cells outside this volume. The CTV must receive adequate dose to achieve the therapeutic aim.
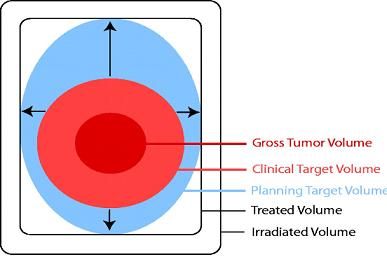
Figure (a) shows the ICRU 50 measurements volume
Internal Target Volume:
ICRU Report no. 62 (25) recommends that an internal margin (IM) be added to CTV to compensate for internal physiologic movements and variation in size, shape, and position of the CTV during therapy in relation to an internal reference point and its corresponding coordinate system. The volume that includes CTV with these margins is called the internal target volume (ITV).
Planning Target Volume:
The volume that includes CTV with an IM as well as a setup margin (SM) for patient movement and setup uncertainties is called the planning target volume (PTV). To delineate the PTV, the IM and SM are not added linearly but are combined rather subjectively. The margin around CTV in any direction must be large enough to compensate for internal movements as well as patient motion and setup uncertainties.
Planning Organ at Risk Volume:
The organ(s) at risk (OR) needs adequate protection just as CTV needs adequate treatment. Once the OR is identified, margins need to be added to compensate for its movements, internal as well as setup. Thus, in analogy to the PTV, one needs to outline planning organ at risk volume (PRV) to protect OR effectively. Figure (b) schematically illustrates the process of outlining PTV and PRV. This process is intended to make the radiation oncologist think methodically and analytically when outlining targets and organs at risk instead of taking a wild guess. Although absolute accuracy in either case cannot be assured, the objective of this approach is to minimize errors by paying attention to details.
It is also important to point out that there is a common tendency among practitioners to draw target volumes based on GTV with little margins to account for subclinical disease, organ motion, or setup uncertainties. The so-called conformal radiation therapy is a double-edged sword—a high degree of plan conformity can create a high probability of geographical miss. Thus, great caution must be exercised in designing PTV and PRV. It is just as important to know the limitations of the system as it is to know its capabilities.
Treated Volume:
Additional margins must be provided around the target volume to allow for limitations of the treatment technique. Thus, the minimum target dose should be represented by an isodose surface that adequately covers the PTV to provide that margin. The volume enclosed by this isodose surface is called the treated volume. The treated volume is, in general, larger than the planning target volume and depends on a particular treatment technique.
Irradiated Volume:
The volume of tissue receiving a significant dose (e.g., ≥50% of the specified target dose) is called the irradiated volume. The irradiated volume is larger than the treated volume and depends on the treatment technique used.
Maximum Target Dose:
The highest dose in the target area is called the maximum target dose, provided this dose covers a minimum area of 2 cm2. Higher dose areas of less than 2 cm2 may be ignored in designating the value of maximum target dose.
Minimum Target Dose:
The minimum target dose is the lowest absorbed dose in the target area.
Mean Target Dose:
If the dose is calculated at a large number of discrete points uniformly distributed in the target area, the mean target dose is the mean of the absorbed dose values at these points. Mathematically:

Where N is the number of points in the matrix and Di, j is the dose at lattice point i, j located inside the target area (AT).
Median Target Dose:
The median target dose is simply the value between the maximum and the minimum absorbed dose values within the target.
Modal Target Dose:
The modal target dose is the absorbed dose that occurs most frequently within the target area. If the dose distribution over a grid of points covering the target area is plotted as a frequency histograph, the dose value showing the highest frequency is called the modal dose.
Hot spot:
A hot spot is an area outside the target that receives a higher dose than the specified target dose. Like the maximum target dose, a hot spot is considered clinically meaningful only if it covers an area of at least 2 cm2.
Questions:
1. Clinical Target Volume includes,
a) Gross tumour volume
b) Exact tumour volume
c) Gross tumour volume plus microscopic spread
d) All
2. Which report suggest that Internal Margin should be added to the CTV?
a) ICRU 50
b) ICRU 62
c) ICRU 55
d) ICRU 60
Answer:
1. c) Gross tumour volume plus microscopic spread
2. b) ICRU 62
References:
1. http://jicru.oxfordjournals.org
2. The Physics of Radiation Therapy by F. M. Khan
Home > Treatment Planning > Prescription & Dose Calculation > Treatment Prescription > Treatment Volume
Can we please get your advice on this one question?
FREE Infographic What successful people believe. What successful people do
Dictionary of Cancer Terms
Need help understanding a word? Here is an electronic resource that gives meaning to Cancer terms and their usage.
StrengthsFinder 2.0